
I know because I have worked in several senior NHS positions and have seen it first-hand. It works like this…..
- All major NHS institutions from NHS England down are managed by a board consisting of Executive Directors (EDs) who do the actual work and Non-Executive Directors (NEDs) who are there to hold them to account.
- The EDs are appointed by the NEDs, who also have the power to remove them if they are not up to the job.
- EDs are required at intervals to provide the board with assurance that things are going well and that if this is not the case that there are plans in place to correct the situation.
- It is essential that the board accepts this assurance. If they are not assured they must report up to their regulator – usually NHS Improvement.
- If they are not assured the easiest action they can take is to get a new ED who will assure them better.
The problem is that the EDs know full well that that rising demand, inadequate funding, a catastrophic manpower plan and health inflation will make it impossible to provide honest assurance to the board, but to say they cannot deliver a safe solution is professional suicide.
On the other hand NEDs cannot afford to hear that there is no safe solution. It means that they have failed and in all likelihood NHS Improvement will replace them.
This is where the rot sets in
All board members know that the real state of affairs but they are not allowed to admit it. Yet they cannot lie, or at least be caught lying, or they will certainly be for the chop. In board meeting EDs choose their words carefully, glossing over the negatives and emphasising the positives. They are overoptimistic about the likely success of recovery plans.
The NEDs don’t believe a word but it is not in their best interest to challenge too hard, especially when is no solution that will be acceptable to the government. Indeed they will often exert considerable pressure on EDs to get them to say what they need to hear. This is where NHS bullying culture originates. NEDs accept the assurance in the knowledge that when it all goes pear shaped they can say they were misled and will have an obvious scapegoat to blame.
So boards are made up of intelligent people who know the score but can’t see a solution, who dance round their handbags misleading each other, desperately hoping they will make it to retirement or the next job before it all falls apart.
This climate of deceit and bullying filters down to middle management and ultimately poisons the whole NHS.
They tend not to lie on paper because that can be more easily challenged. They have to put the facts in the board papers but hide them in a sea of “boardspeak” platitudes.
If you don’t believe me take a look at this image.
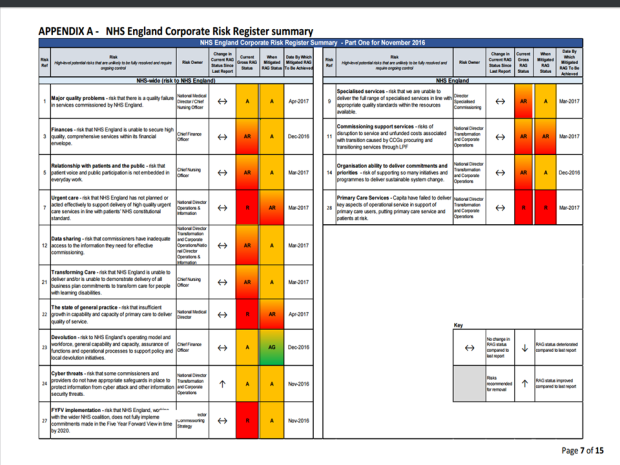
It is the risk register taken from the NHS performance report presented to the last NHS England board meeting in December 2016. It is a sea of red and amber risks which cover almost all areas of NHS service. Things do not seem to be improving and there is no sense that the mitigation plans will make much difference.
Then read the board paper from which this table is taken. It glosses over this appalling situation. (I know you won’t read it but believe me it is a bit limp to put it mildly).
Now have a look at this recording of the part of the board meeting where the paper was discussed. Most of you will not have seen this. Indeed at the time of publishing this blog only 53 people have bothered to watch it. It is twenty four minutes long but you will get the gist after 2 minutes. It is really worth doing the first 10 minutes if you want to get your blood boiling as they start to talk about the emergency department crisis.
I was reminded of this culture by Professor Jane Cummings latest missive about closing beds to free up cash for social care. She cannot really believe this will work when we have fewer beds and doctors per head of population than almost anywhere else in Europe. She is spinning the current lie that NHS England board members are deluding themselves with in order to keep her job.
So we seem to have the appalling situation where everyone at the top of the NHS knows that it is falling apart but in order to keep their jobs they have to reassure each other and their political masters that everything is fine. In the meantime the NHS is going to the dogs, clinicians are burning out and patients are suffering.
We desperately need senior people in the NHS to admit what is happening. I hope this will start with clinical board members – Medical and Nursing Directors in particular. They have duty to protect patients under their respective professional codes of practice.
It is about time for them to grow a backbone, and to speak out – before it is too late.

Yes! Blood pressure now at dangerous levels!
LikeLike
“Focus heavily [sic]… on Capita..”
Oh happy day…
LikeLike
Youssef El-Gingihy the author of ‘How to dismantle the NHS in 10 easy steps was on the 12.00 O-clock news today, they gave him a good airtime and he told it like it is, but I don’t know if it was repeated on the main evening news.
LikeLike
Illuminating – thank you.
This resonates because I’ve just been re-reading Neville Shute’s autobiography and will share some here. He was an engineer involve in work on the airship being developed in parallel to the disastrous R101 and later in the Admiralty during the war. Shute’s considered analysis of the root causes of he R101 disaster is that none of the officials in government could risk their jobs by going against the directive from the Secretary of State that all was well, and all had to be well as he was staking his political career on (although ironically he was one of the 36 who died in the consequent tragedy). “Perhaps it is easy for an engineer to write like this, for he can get another job without much difficulty in some other branch of engineering: perhaps it is even easier for an author. That should not blind us to the facts, however, that in this case a number of high civil servants shirked their duty to preserve their jobs. It may be that under modern conditions of life in England it is unfair to expect a man who has spent his life in government service and is unfitted for any other occupation to place his duty to the State before his job. But if that be so, it should be clearly realised that in certain circumstances these high civil servants will not do their duty, though all the honours in the book be showered on them by the Crown.”
Shute also writes of his work in the Admiralty in wartime – when you sometimes needed quick decisions and it was a pleasure to deal with those who would authorise public expenditure on the basis of a conversation – with the paperwork and releases to follow in due course. “Now and again, we would find some cheerful young commander or captain who was not affected by these scruples, who was as brave in the office as he was at sea. Commenting on such a regular officer and on his way of doing business we would say, ‘He’s a good one. I bet he’s got private means.’ Invariably investigation would prove us right. The officers who were brave in the Admiralty were the officers who had an independent income, who could afford to resign from the Navy if necessary without bringing financial disaster to their wives and children. … These were the men who could afford to shoulder personal responsibility in the Admiralty, who could afford to do their duty to the Navy in the highest sense.”
And he brings the two together: “I do not know the financial condition of the high officials in the Air Ministry at the time of the R101 disaster. I suspect, however, that an investigation would reveal that it was England’s bad luck that at that time none of them had any substantial private means. At rock bottom, that to me is probably the fundamental cause of the tragedy.”
LikeLiked by 1 person
Great writer to boot. However, what these craven lickspittles also conspire with is to punish the NHS whistle blowers. A very sad and frightening state of affairs.
LikeLiked by 1 person
Of course many are hoping to be in situ when the great privatisation occurs, as they will be rewarded handsomely. We all know the secret of private sector ” success” is in managing your managers, not actually being responsible for anything yourself.
LikeLike
This is an entirely accurate account of my own professional experience, this is truly a clear and transparent articulation of the reality, Wonderful
LikeLike
Reblogged this on redbridgetradeunionparty.
LikeLike
Mmm, I did watch most of the NHSE board mtg part as suggested above re NHS performance report. I was underwhelmed by the large amount of patient blaming, stating the bleeding obvious, BUT lack of strategic discussion by the board. Luckily, I’m managing my own high blood pressure as awaiting a GPs appt to discuss this. Therefore, decided to not watch all of this clip for the sake of my health…
LikeLike
I think it is worse than this piece suggests. I think they are all actively coluding in shaping the NHS up for a US style privatisation. The US has the worst medical system in the world. It does however prove lucrative to whose who make a profit from it.
It is noticeable that NHS Scotland and NHS Wales are not doing STP cuts packages and they didn’t implement the junior doctors’ contract.
LikeLiked by 1 person
Practical common sense, trust, care and honesty should be the key factors that any current or future EDS / NEDS should have. And furthermore stop sticking a plaster over everything and speak up and let the government hierarchy know what’s happening under their noses, it’s not rocket science.
BTW, lovely blog and good to hear from someone who cares.
LikeLike
add to this ‘reassurance’ isn’t needed at this level. Reassurance absolutely belongs on the ground floor, where your comforting relatives and letting them know your doing everything you can or you might say reassuring your patient and their loved ones.
At board level however, perhaps it’s time to stop asking for reassurance and start asking for evidence. Questions like ‘how do you know?, ‘what evidence do you have that makes you think that approach will work?’
LikeLike
Reblogged this on Jaffer's blog.
LikeLike
The NHS is essentially a socialist institution (free health care for everyone) that is totally dependent on a capitalist economy and ethos, which condemns it to certain failure.
Along with the welfare state, the NHS was founded in the aftermath of WW2 on the assumption of a widely shared sense of national identity and social solidarity. At the time, this assumption was justified. But not any more. Britain is not a nation, but a mercenary “patron state” deceitfully posing as a nation, in order to legitimise itself, its ruling elites and the immense power they wield and abuse.
Why is this not recognised by the academics we look to as authorities in understanding society and the state? Like their medieval predecessors and counterparts, academics are themselves privileged clients and employees of the state, with a massive personal self-interest (subconscious more than conscious) in rationalising and defending its role, self-image (as our “nation”) and ideologies (social, political, economic and racial, formerly religious), on which the state bases its claim to moral and knowledgeable authority.
LikeLike
Stupidity cannot be easily overcome; the higher up the chain of command you go, it’s normal. Too many nodding donkeys at the same time.
LikeLike
Playing the devils advocate, perhaps, but since 1946 life expectancy has increased from 70 to 85, perinatal mortality has decreased from 40/1000 to about 3/1000, and heart disease has now been replaced by dementia as a leading cause of death.
Smoking rates have dropped from 50% to below 25%.
As for Priority Care services, around 400,000 people no longer live in the gulag of Victorian asylums.
So it isnt all bad…
LikeLike
Need to strip it all back and get back to basics, that means listening to the staff on the front line and then taking action.
Put all the nodding dogs out to pasture.
The above all seems too easy, but hey miracles can happen, can’t they?
LikeLike
The bit about ‘make a GP appointment instead of going to A&E’ is laughable in some areas. My 90yo mother’s practice has a system of ‘call from 8am to make a same day appointment’ (until the appointments for that day run out, then you are turned away) or it’s an 8 week wait to see anyone. She rarely gets up before 8:30 by which time all appointments have gone. My own practice is fantastic however – 7-10 day wait for appointments, and all day duty doctor service with end-of-day appointments held for these cases. Online information systems don’t work for older people. I don’t know how these people sit in these meetings and just play along with the game. Gloss over the figures, push patients in alternative directions (without really having much evidence that they work) and then (presumably) spend a lot of money advertising these routes which could be directed towards core services.
LikeLike
The old addage “only good news goes up the chain/ rises” was most probably invented by nhs workers as this is endemic from mid mgt upwards, also if you were inept or skilled at dodging bullets then you were promoted through mgmt, it is a no blame culture, that is disease ridden with job protecting beaurocrats who quite frankly operate like a bunch of candidates from the apprentice, and seek to keep a handle on their budgets by denying progress and restricting replacement of equipment and resources
LikeLike
Reblogged this on NHAspace and commented:
A clear insight into the way NHS England try to gloss over what’s happening to the NHS. This is why we cannot allow politicians to shirk their duty to provide a functional NHS.
LikeLike
Matthew Swindel,s talking about emergency care. Pretty much anyone in NHS management could have said the same thing after 5 minutes research to get the stats he quotes. So much for the NHSE expertise. And I have heard exactly the same lines In a number of Boards over the past decade. Clearly it’s not working, so why flog a dead horse.
LikeLike
Their working manual must be ‘the emperors new clothes’ in an NHS cover
LikeLike
Infested with psychopaths.
LikeLike
Wow, that vid. Is the woman paid on commission for the word positive?
LikeLike
Thanks for the story concerning %BT%? It sounds delicious to provide a some of it and discuss
it! I plan to read more particulars about this situation for my web site!
LikeLike